
Chapter 19: CPT Evaluation & Management Section Workbook Case 5 Answers and Rationale.
NEW PATIENT OFFICE VISIT |1|
CHIEF COMPLAINT: Right lower quadrant abdominal pain. |2|
HISTORY OF PRESENT ILLNESS: The patient is a 67-year-old who presents with diffuse right lower abdominal pain. |3| The pain tends to be located near his right groin. He states that it has been present since the summer of 20XX. He was doing some significant activity at that time, including significant manual labor in his yard. It was at that time that he began to notice the symptoms. He continued to work in construction throughout the summer and fall. His symptoms continued through this time and only recently, as he has limited his activity, has the pain improved. He does not have any obstructive symptoms. He has not had previous inguinal hernia repair. He was seen by his primary care provider who thought he may have a spigelian type hernia and thus he has been sent to my clinic for evaluation of this problem.
PAST MEDICAL HISTORY: Low back pain, osteoarthritis, hypertension, and anxiety.
PAST SURGICAL HISTORY: Anal fistulotomy, appendectomy, patent foramen ovale closure, multiple arthroscopies, carpal tunnel release bilaterally, hand surgery for tendon releases, and bilateral cataract extraction.
ALLERGIES: He gets nausea and vomiting with narcotics, but otherwise has no true medication allergies.
CURRENT MEDICATIONS: Clonazepam, AndroGel, multivitamins.
FAMILY HISTORY: Noncontributory.
SOCIAL HISTORY: The patient is retired. He tries to exercise regularly. He does not smoke or drink.
REVIEW OF SYSTEMS: An 11-point review of systems was undertaken and, except for some mild upper respiratory tract infection type symptoms and some low back pain, was essentially negative.
PHYSICAL EXAMINATION: Vital Signs: Temperature is 96.4. Heart rate is 72. Blood pressure is 164/92. Respiratory rate is 15. Height is 5 feet 0 inches. Weight is 199 pounds. HEENT: The sclerae are anicteric and the oropharynx is clear. Neck: No jugular venous distension or lymphadenopathy. Chest: Clear to auscultation bilaterally. Cardiac: Regular rate without murmurs. Abdomen: Soft, nontender, and nondistended with no palpable intraabdominal abnormalities of note. Specifically, there are no palpable anterior abdominal wall fascial abnormalities of note. Back: No CVA tenderness and no spinal abnormalities. Groin: Both the right and left inguinal regions are intact with no evidence of hernia. There are no spermatic cord or testicular abnormalities. Extremities: No clubbing, cyanosis, or edema.
ASSESSMENT: Right groin pain, improving with limitation of activity.
PLAN: This patient most likely has one of two issues that are responsible for his symptoms. |4| One would be an occult hernia on the right side. This would present with pain without a palpable hernia on examination. This is where the posterior wall is disrupted and can lead to the same symptoms as an inguinal hernia, but without a palpable hernia. In this situation, patients typically do not get very much relief of their symptoms by decreasing their activity as one is continually utilizing the abdominal wall musculature and remain symptomatic from the hernia. Treatment would require laparoscopic surgery. |5| The other possible pathology would be an abdominal wall injury such as a muscle pull or strain. This typically would get better with rest and since the patient is stating that his symptoms have improved over the last month or so with decreasing his activity then I would expect that he would continue to improve with conservative management. The patient agrees with the plan of continued decreased activity for the next four to eight weeks. |6| He has not had any projects planned around his house and is not going to participate in construction at this time. He will get back to his normal activity in March. He will pay attention to his symptoms and if he does have recurrence of his symptoms with increasing physical activity, he will contact my office to arrange follow up.
|1| This is a new patient.
|2| Chief complaint.
|3| Specificity of the location of the pain, which is required for the diagnosis.
|4| Although the provider has two differential diagnoses, neither is at a high risk of morbidity.
|5| Possible surgical treatment option.
|6| Conservative treatment if rest is chosen.
What are the CPT® and ICD-10-CM code(s) reported?
CPT® code: 99203
ICD-10-CM codes: R10.31
Rationale:
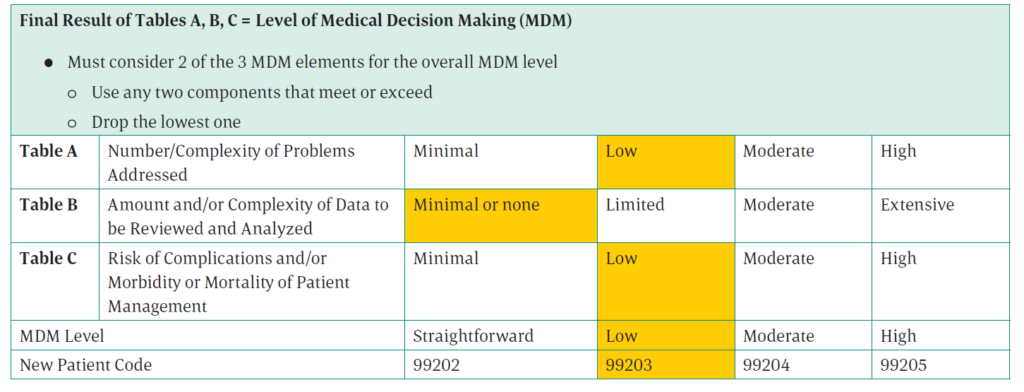
CPT® code: Subcategory — Office visit, new patient, coded using 2021 E/M guidelines
Number and complexity of problems addressed: The provider believes this is one of two problems, neither of which have a high risk of morbidity. This is an acute, uncomplicated illness or injury which results in low for the number and complexity of problems addressed.
Amount and complexity of data to be reviewed and analyzed: There is no data to be reviewed, making this none for the amount and complexity of data to be reviewed and analyzed.
Risk of complications and morbidity or mortality of patient management: The patient’s options are minimally invasive laparoscopic surgery or rest. Regardless of which is chosen, both are taken into consideration for the risk. This makes the risk level low.
ICD-10-CM codes: The diagnosis is right groin pain. Look in the ICD-10-CM Alphabetic Index for Pain/groin and you are directed to see Pain, abdominal, lower. Look for Pain/abdominal/lower/right quadrant and you are directed to R10.31. Verify the code in the Tabular List.